NegotiateIQ — CareFirst BlueCross BlueShield
A negotiation intelligence platform that transforms complex payer contracting data into real-time financial modeling and clinical decision support for CareFirst contracting leaders.
Guidehouse AI Studio – Health (Commercial) · CareFirst · 2026
Overview
Static reporting wasn't built for a negotiation room
- CareFirst's contracting leaders needed live financial modeling, peer benchmarking, and clinical cost intelligence — all during active payer negotiations
- Their existing experience was dense static reports — no scenario modeling, no real-time recalculation
- I designed two interconnected modules — Financial and Clinical — within the GH Design System, adapted for CareFirst
- Delivered in seven days with the developer shipping the same day I produced screens
The Conditions
Seven days. Zero requirements. New client, live negotiations.
CareFirst was a new client. The advising team was new to me. No written requirements, no prior product direction — just a kickoff call and a stakeholder demo already on the calendar.
0
Day sprint
0
Written requirements
0
Core modules delivered
- Role
- Lead Product Designer
- Scope
- Financial & Clinical Dashboards
- Team
- PM, Health SMEs, directors & partners, developer
- Design System
- GH DS — adapted for CareFirst demo
My Role
Holding the bar on product thinking
The advising team kept defaulting to PBI-style outputs and static advising sheets. I was there to demonstrate what a real product looks like in this context.
- Push back when the instinct was to revert to deck mode
- Define MVP scope simultaneously with building it — no sequential planning
- Navigate a domain I didn't deeply know — healthcare payer contracting — fast enough to make design decisions that held up
- Keep the design bar while the team figured out what being a product team meant
“We had no written requirements and a stakeholder demo in seven days. I had a kickoff call, a rough idea of the problem space, and a developer ready to ship the same day.”
Daily cadence
- Morning — alignment call with PM, SMEs, and developer
- Midday — screens designed and reviewed in the same session
- Afternoon — developer ships; feedback collected from stakeholders
- Repeat — every day for seven days
Approach
Structured around a negotiation workflow
Rather than designing individual screens, I structured the experience around the decisions a contracting leader must make: before, during, and after a negotiation.
Set Context
Scope the analysis to the correct facility and population before entering any financial view.
Assess Financial Position
Evaluate current reimbursement, peer benchmarking, and rate impact with a single editable sensitivity lever.
Drill Down to Build a Target
Navigate from service category to DRG level to identify which lines to adjust to reach a financial target.
Identify Clinical Cost Drivers
Uncover utilization patterns and avoidable spend that strengthen negotiation positioning.
Set Context in Practice
Global filter
Before entering any financial view, leaders scope the analysis to the correct facility and population. This prevents misaligned data from entering the conversation.
Financial Analysis
Three layers of financial intelligence
Structured into three cognitive layers for rapid scanning in a live negotiation room:
- Summary Metrics — Current Reimbursement, Rate Impact, Clinical Opportunity, Net Impact
- Peer Comparison — Facility % of Medicare vs. peer benchmark for inpatient and outpatient
- Scenario Modeling — Single input recalculates downstream impact dynamically
- Historical Trend — Quarterly % of Medicare for facility vs. peer over time
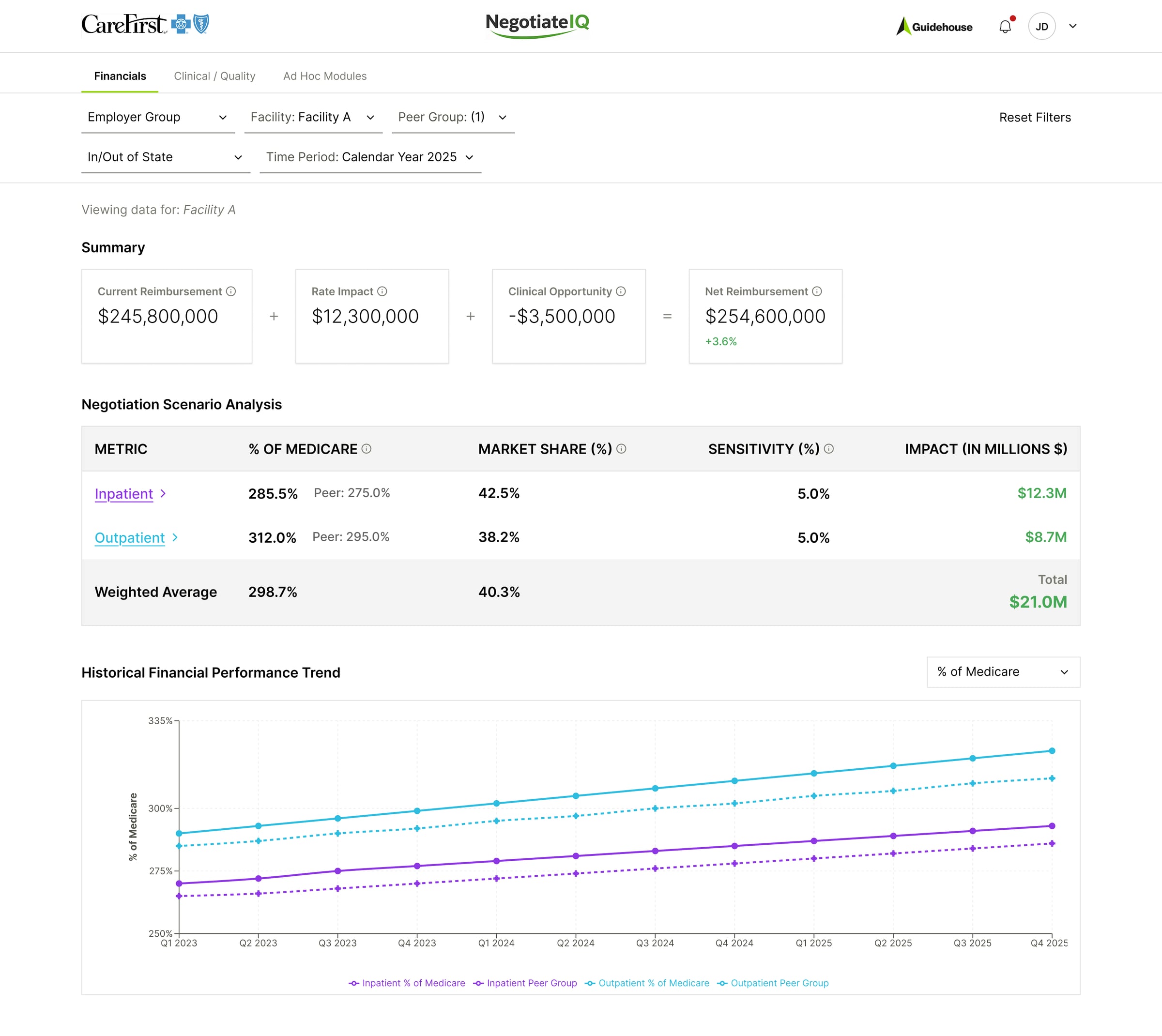
Financial overview — three-layer layout for rapid scanning
Scenario Modeling
Real-time sensitivity in the room
- Single input — a percentage slider (0–20%)
- Instantly recalculates rate impact across all downstream metrics
- Simple enough to operate mid-conversation without breaking flow
Drill-Down Architecture
From summary to DRG level in three clicks
The hierarchy follows how contracting teams think:
- Service Category → Service Line → DRG (inpatient) or CPT (outpatient)
- Negotiation target pinned top-right as a persistent reference
- Each row: facility % of Medicare, peer benchmark, market share, sensitivity %, dollar impact
- Adjustments at any level roll up dynamically — users build position bottom-up
Drill-Down Screens
Designed to stay in the room
In a live negotiation, losing your place breaks momentum. The drill-down expands in place — no modals, no page changes. A leader moves from category to DRG and back without losing context.
Collapsed
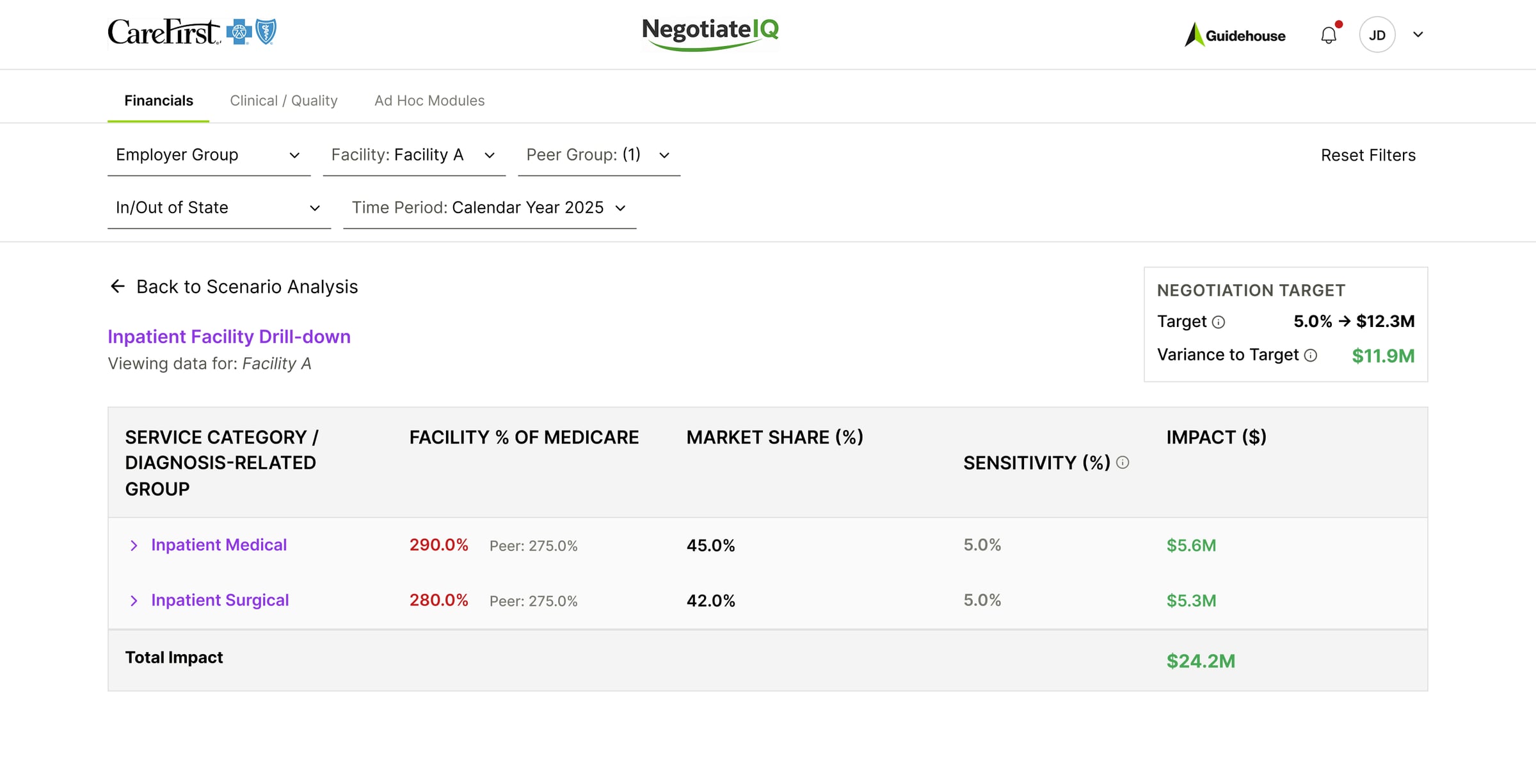
Inpatient — collapsed by service category
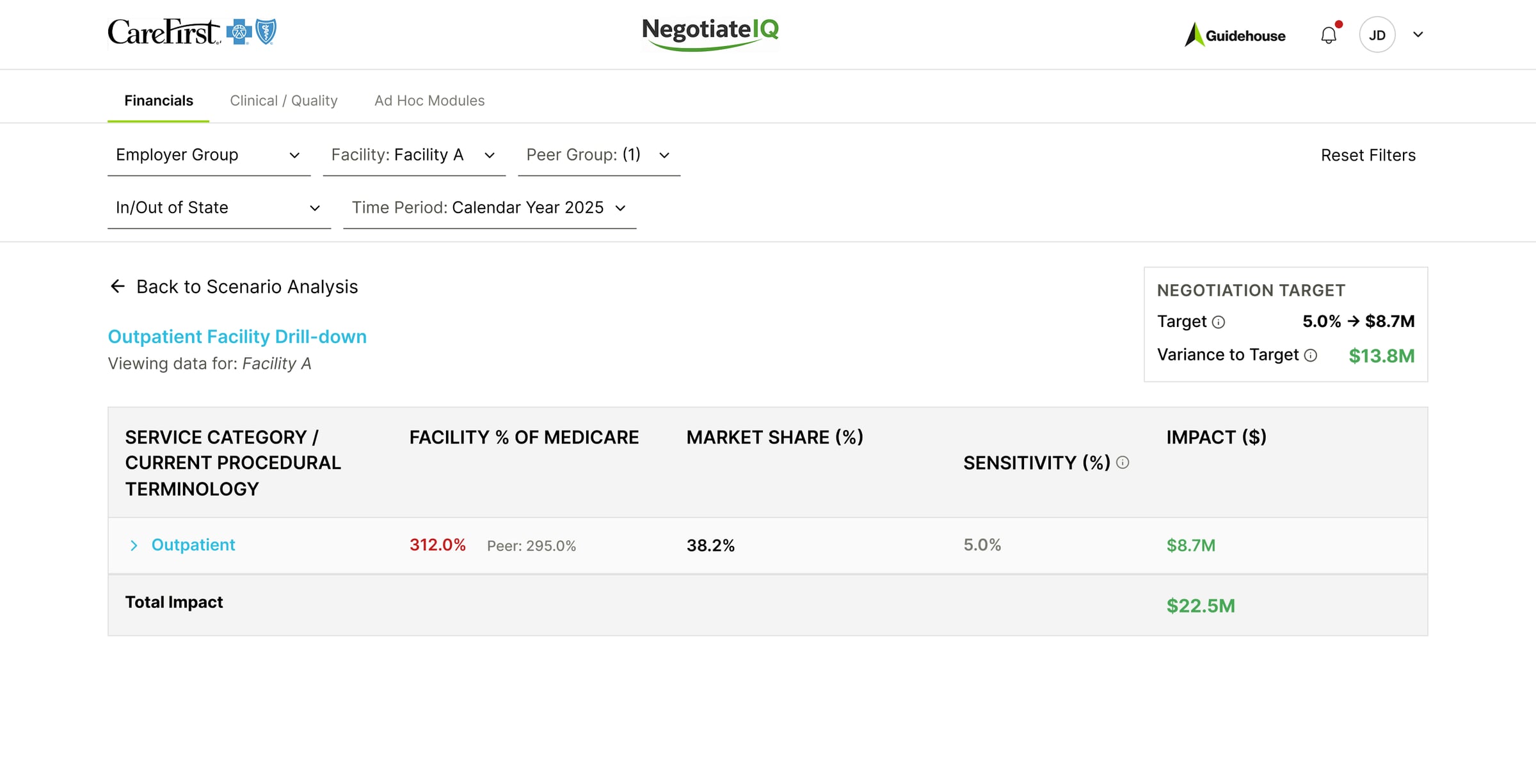
Outpatient — collapsed by service category
Expanded
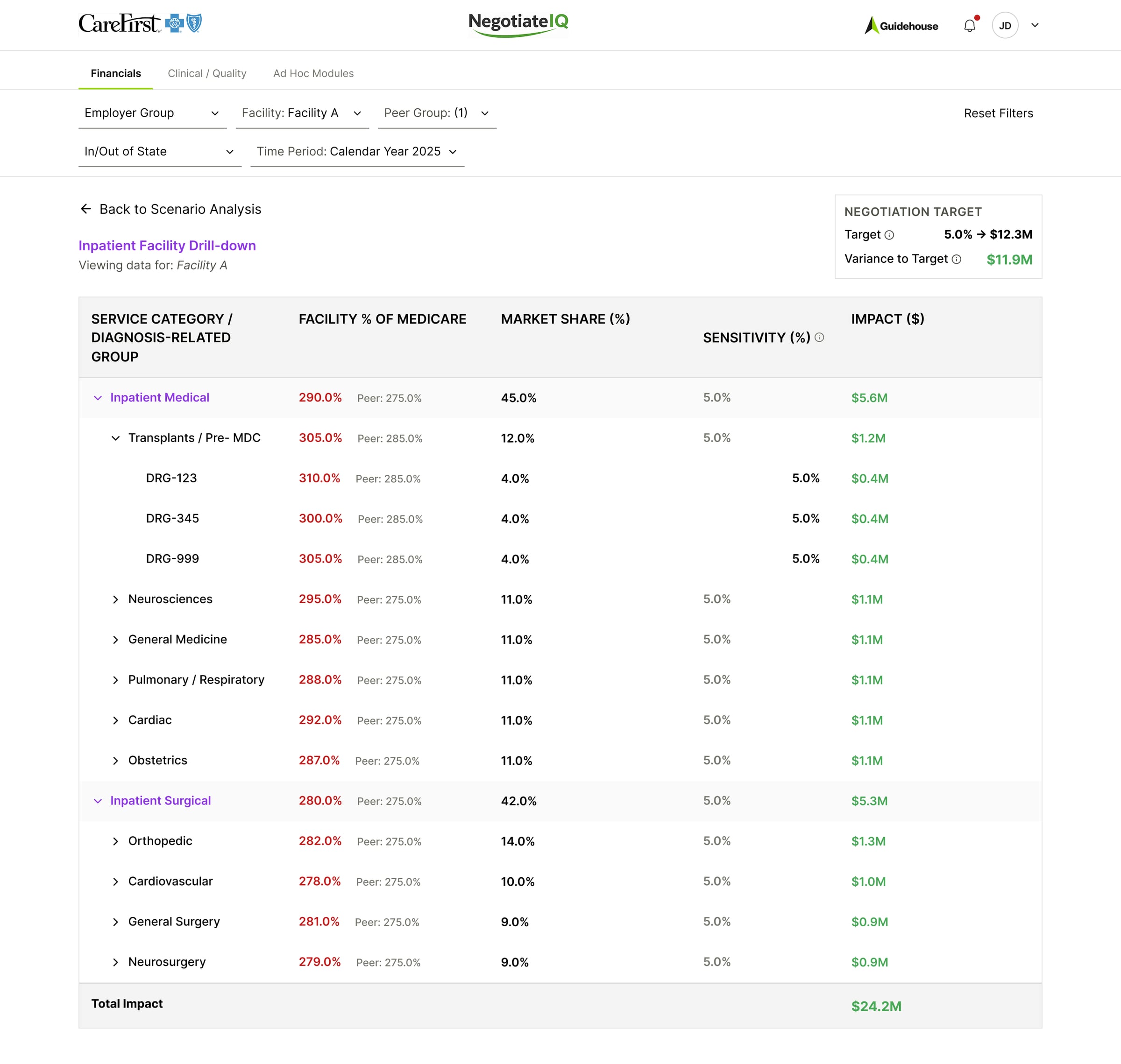
Inpatient — expanded to service line and DRG
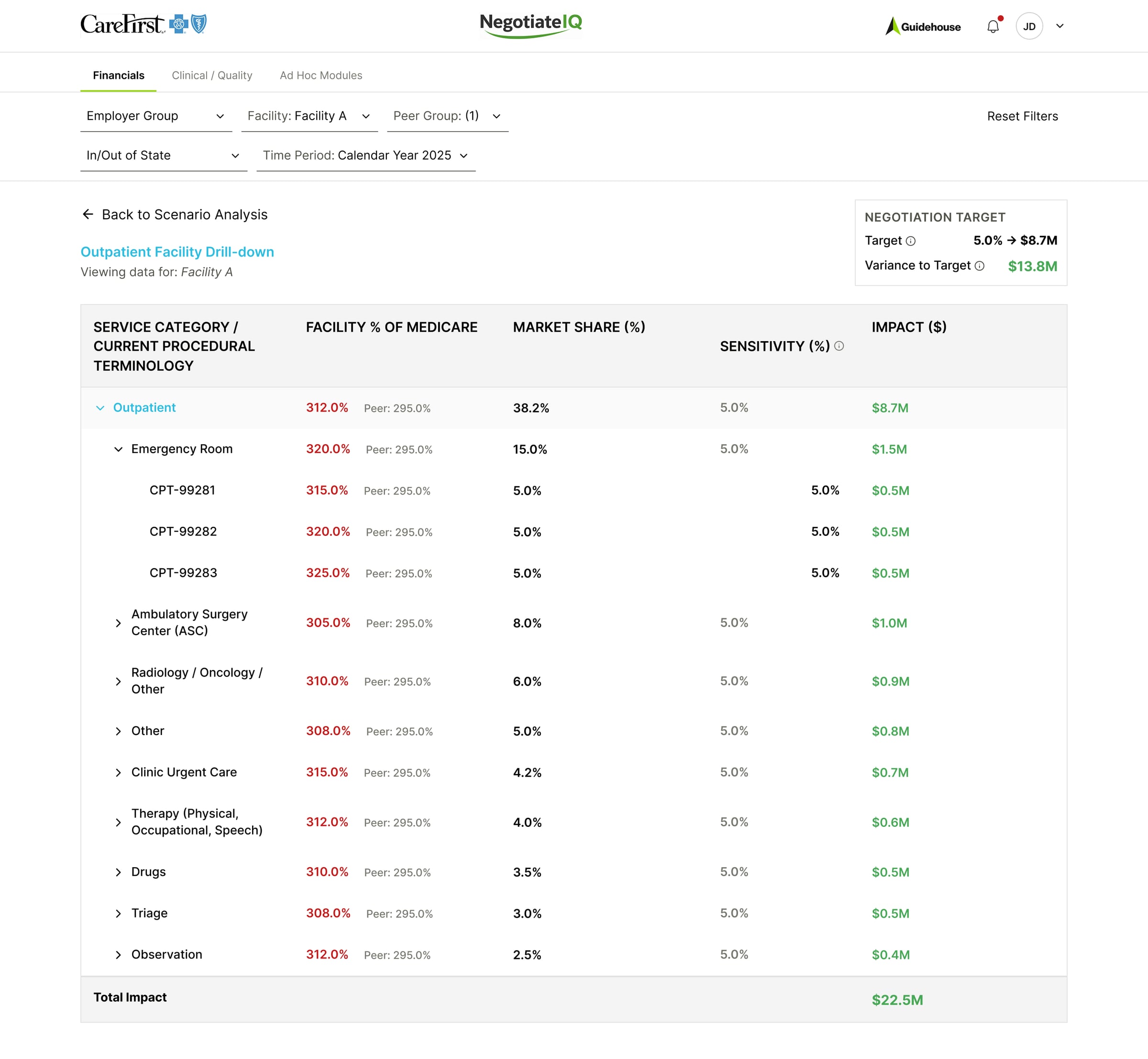
Outpatient — expanded to service line and CPT
Clinical Intelligence
Cost drivers that strengthen positioning
The Clinical dashboard surfaces performance signals that directly inform negotiation strategy:
- ALOS (CMI adjusted), Readmission Rate, Mortality
- Potentially Avoidable Admissions and Avoidable ED Visits
- Percentages, counts, and spend clearly differentiated — with quarterly trend on hover
- Drill-down available only where the data justifies it
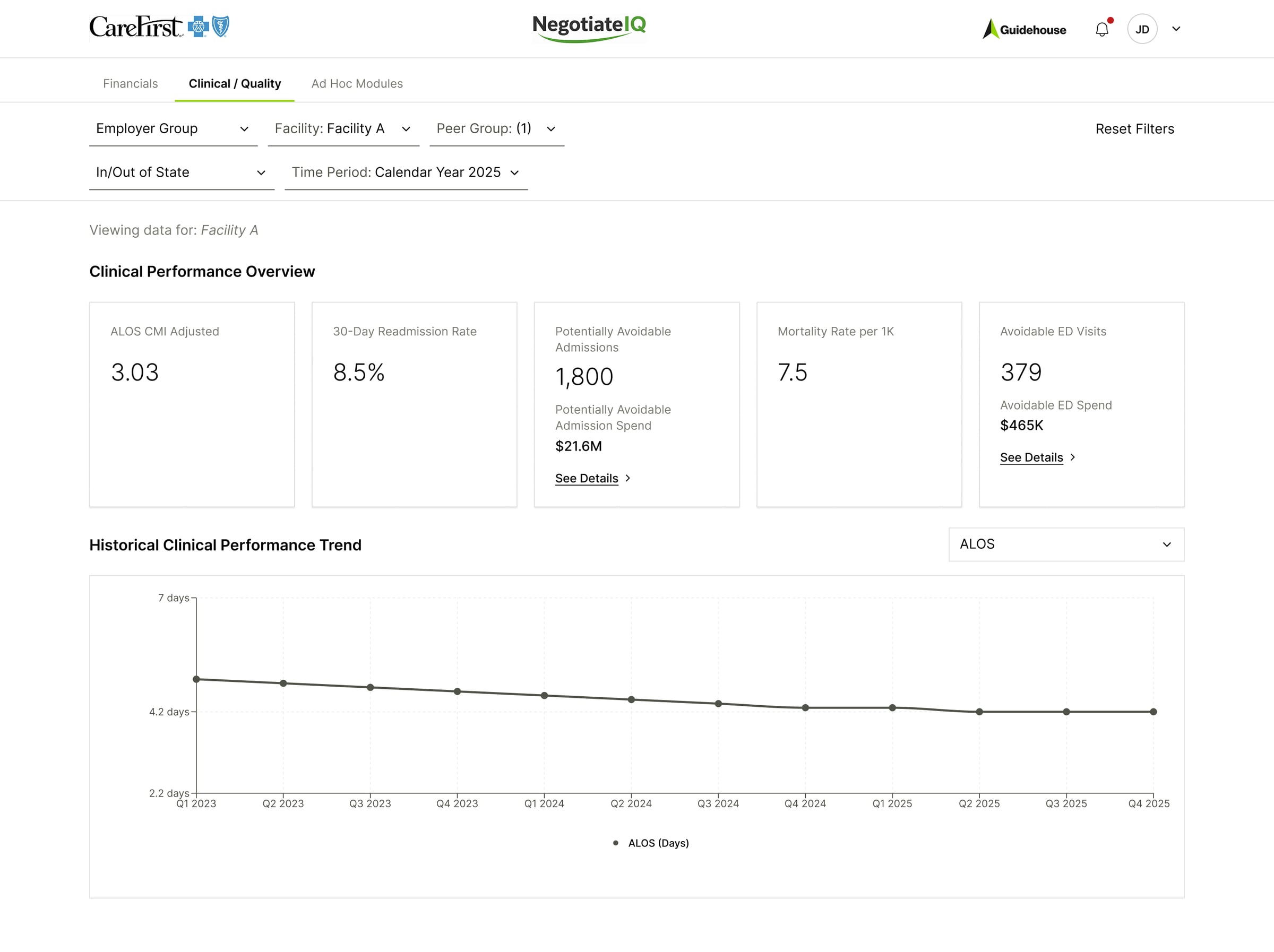
Clinical overview — key performance signals with selective drill-down
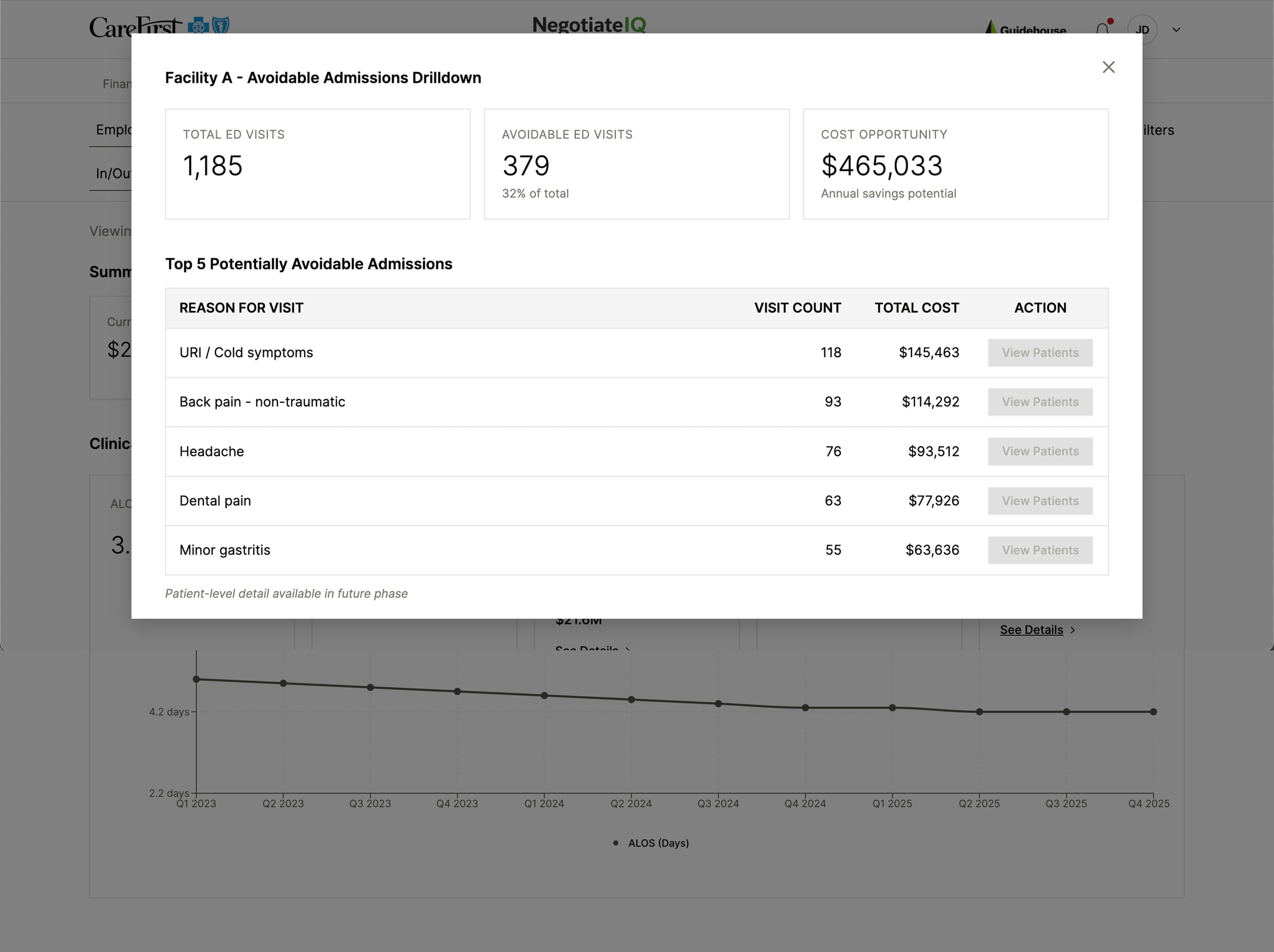
Clinical Drill-Down
From signal to cost driver in two clicks
- Total visits and the avoidable subset
- Annualized savings potential
- Top 5 reasons by visit count and total cost
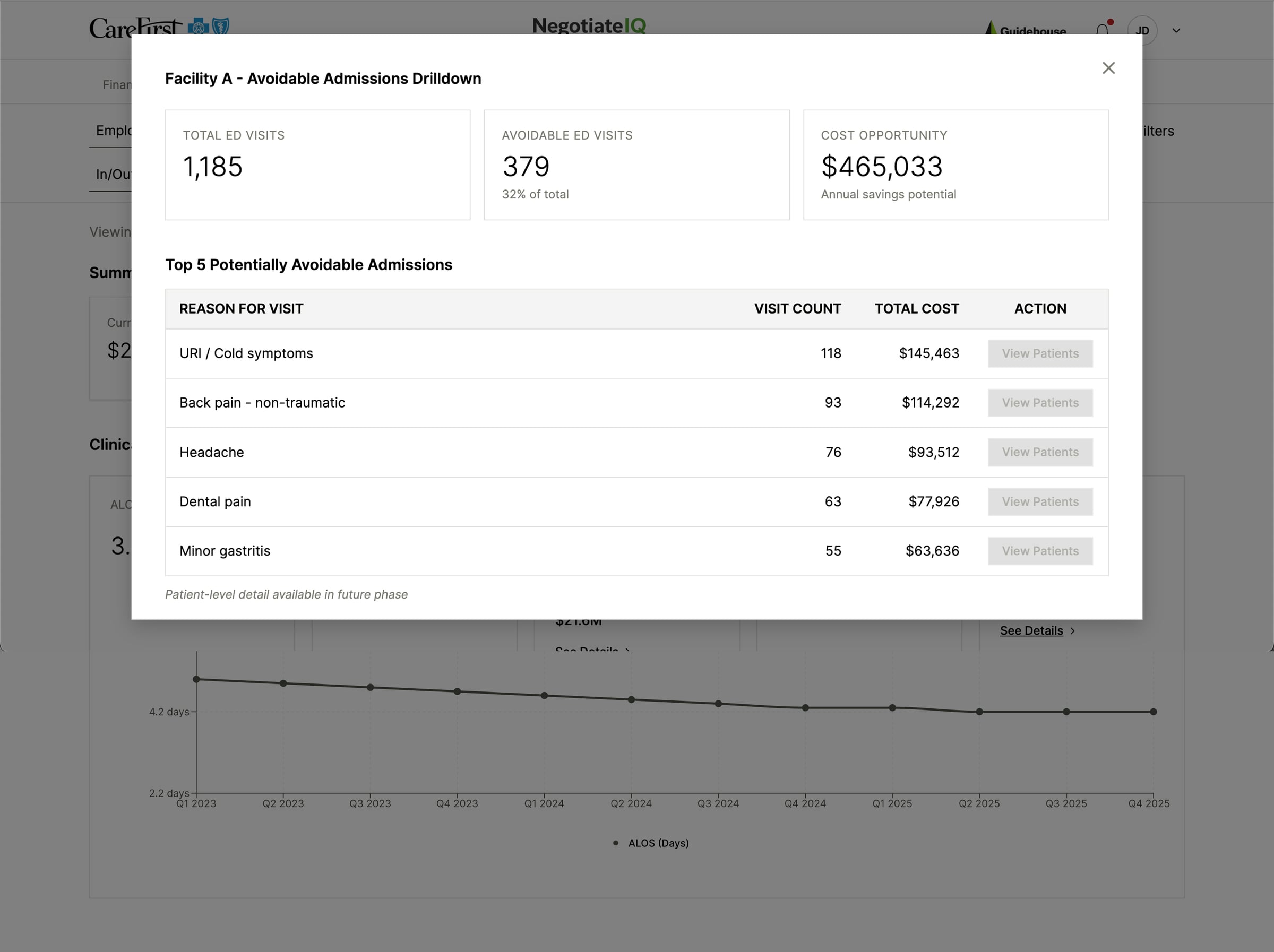
Cost Signal
Pinpointing avoidable spend
- Total ED visits and the avoidable subset
- Annualized savings potential surfaced immediately
- Top 5 avoidable reasons by visit count and cost
- “View Patients” placeholder for a planned future phase
Whatthisprojectdelivered
- Transformed static financial outputs into interactive negotiation workflows
- Enabled real-time scenario modeling usable during live executive discussions
- Reduced ambiguity in peer comparisons with structured % of Medicare benchmarking
- Created scalable drill-down architecture from service category to DRG and CPT level
- Surfaced clinical cost drivers that directly support negotiation positioning
- Delivered two production-ready modules in seven days with zero written requirements
Reflection
Design for high-stakes decision environments
Every decision — the three-layer financial layout, the bounded drill-down hierarchy, the sensitivity lever, the clinical signal selection — was made in service of one environment: a live negotiation room where clarity is the product.
What made this project rare was the conditions. Seven days, a new client, a team finding its product footing, and a scope written the same week it was built. That kind of environment sharpens everything fast.